
Prostate Cancer & how to deal with it!
Prostate Cancer only happens with men, because the Prostate is part of the male reproduction system.
About 99% of cases occur in those men over the age of 50.
Globally it is the second most common type of cancer and the fifth leading cause of cancer-related death in men.[1]
Prostate cancer rates are higher and survivals are poorer in developed countries than in the rest of the world. Many of the risk factors for prostate cancer are more prevalent in the developed world, including longer life expectancy and diets high in red meat. (People who consume larger amounts of meat and dairy also tend to consume fewer portions of fruits and vegetables. It is not currently clear whether both of these factors, or just one of them, contribute to the occurrence of prostate cancer.[2]) Also, where there is more access to screening programs, there is a higher detection rate. Prostate cancer is the ninth-most-common cancer in the world, but is the number-one non-skin cancer in men from the United States.
Prostate cancer is diagnosed by biopsy.
Prostate cancer screening is controversial.[3][4] Prostate-specific antigen (PSA) testing increases cancer detection but does not decrease mortality.[5] The United States Preventive Services Task Force recommends against screening using the PSA testing, due to the risk of over-diagnosis and over-treatment as most Prostate cancer presently diagnosed would remain unknown with no symptoms.
Many cases can be safely followed with active surveillance or watchful waiting. Other treatments may include a combination of surgery, radiation therapy, hormone therapy or chemotherapy.[6] When it only occurs inside the prostate it may be curable.[4] Outcomes depend on a person’s age and other health problems as well as how aggressive and extensive the cancer is.
Most people with prostate cancer do not end up dying from the disease.[6]
Studies of males who died from unrelated causes have found prostate cancer in 30% to 70% of those over age 60.[4]
Early prostate cancer usually causes no symptoms. Sometimes, however, prostate cancer does cause symptoms. These include frequent urination, increased urination at night, difficulty starting and maintaining a steady stream of urine, blood in the urine, and painful urination. A study based on the 1998 Patient Care Evaluation in the US found that about a third of patients diagnosed with prostate cancer had one or more such symptoms, while two thirds had no symptoms.[7]
Prostate cancer is associated with urinary dysfunction as the prostate gland surrounds the urethra tube. (See diagram).
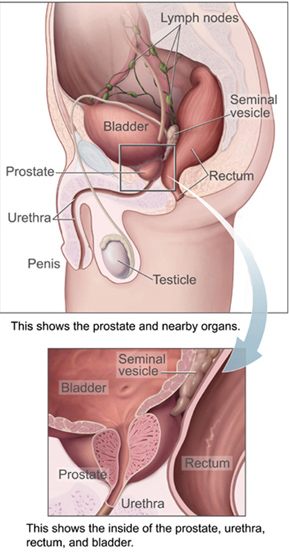
Changes within the gland, therefore, directly affects the ability to discharge urine (pee). Because the tube from the testes deposits seminal fluid into the urethra tube, and secretions from the prostate gland itself are included in semen content, prostate cancer may also cause problems with sexual function and performance, such as difficulty achieving erection or painful ejaculation.[7]
Advanced prostate cancer can spread to other parts of the body, possibly causing additional symptoms. The most common symptom is bone pain, often in the bones of the spine, pelvis, or ribs. Spread of cancer into other bones such as the femur sometimes occurs. Prostate cancer in the spine can also compress the spinal cord, causing leg weakness and bowel and urine leakage.[8]
Risk Factors
A complete understanding of the causes of prostate cancer remains elusive.[9] The primary risk factors are obesity, age and family history. Prostate cancer is very uncommon in men younger than 45, but becomes more common with advancing age. The average age at the time of diagnosis is 70.[10]
However, many men never know they have prostate cancer.
Men who have first-degree family members with prostate cancer appear to have twice the risk of getting the disease compared to men without prostate cancer in the family.[11] This risk appears to be greater for men with an affected brother than for men with an affected father, and those with two first-degree relatives affected have a five times greater risk compared with men with no family history.[12]
Men with high blood pressure are more likely to develop prostate cancer.[13] There is a small increased risk of prostate cancer associated with lack of exercise.[14]
Infection or inflammation of the prostate may increase the chance for prostate cancer while another study shows infection may help prevent prostate cancer by increasing blood to the area. In particular, infection with the sexually transmitted infections, Chlamydia, gonorrhea, or syphilis seems to increase risk.[15] Finally, obesity [16] and elevated blood levels of testosterone [17] may increase the risk for prostate cancer. There is an association between vasectomy and prostate cancer however more research is needed to determine if this is a causative relationship.
Several case-control studies have shown that having many lifetime sexual partners or starting sexual activity early in life substantially increases the risk of prostate cancer.[18][19][20]
On the other hand, while the available evidence is weak,[21] tentative results suggest that frequent ejaculation may decrease the risk of prostate cancer.[22] A study, over eight years, showed that those that ejaculated most frequently (over 21 times per month on average) were less likely to get prostate cancer.[23] The results were broadly similar to the findings of a smaller Australian study.[24]
A study published in January 2015 found that “Among patients with prostate cancer, those who smoke have increased risks of experiencing side effects from treatment and of developing future cancer recurrences, or even dying from prostate cancer”. [25]
In another study published in February 2015 titled “Use of Phosphodiesterase Type 5 Inhibitors May Adversely Impact Biochemical Recurrence after Radical Prostatectomy”,[26] researchers found an adverse association between the use of erectile dysfunction (ED) drugs after radical prostatectomy and biochemical recurrence.
After surgery, about a quarter of the men (23.4%) were treated with a PDE5 inhibitor for Erectile Dysfunction, which is a common complication of the procedure and a known problem in aging men. The drugs used included sildenafil (Viagra), vardenafil (Levitra), and tadalafil (Cialis).
Taking Viagra after prostate surgery likely to cause recurrence.
The researchers said that they were surprised by the findings; they had hypothesized that the drugs would be protective because multiple lab studies and an observational clinical study suggested an anticancer effect in the prostate.
Diagnosis
The American Cancer Society’s position regarding early detection is “Research has not yet proven that the potential benefits of testing outweigh the harms of testing and treatment. The American Cancer Society believes that men should not be tested without learning about what we know and don’t know about the risks and possible benefits of testing and treatment. Starting at age 50, (45 if African American or brother or father suffered from condition before age 65) talk to your doctor about the pros and cons of testing so you can decide if testing is the right choice for you.”[27]
The only test that can fully confirm the diagnosis of prostate cancer is a biopsy, the removal of small pieces of the prostate for microscopic examination. However, prior to a biopsy, less invasive testing can be conducted.
There are also several other tests that can be used to gather more information about the prostate and the urinary tract. Digital rectal examination (DRE) (finger up the bum) may allow a doctor to detect prostate abnormalities. Cystoscopy shows the urinary tract from inside the bladder, using a thin, flexible camera tube inserted down the urethra tube. Transrectal ultrasonography creates a picture of the prostate using sound waves from a probe in the rectum.
In January 2015 a study by the University of Maryland Medical Center found that “Targeted biopsy using new fusion technology that combines magnetic resonance imaging (MRI) with ultrasound is more effective than standard biopsy in detecting high-risk prostate cancer”.[28]
Prevention
Diet and lifestyle
The data on the relationship between diet and prostate cancer is poor.[29] In light of this the rate of prostate cancer is linked to the consumption of the Western diet.[29] There is little if any evidence to support an association between trans fat, saturated fat and carbohydrate intake and risk of prostate cancer.[29][30] Evidence regarding the role of omega-3 fatty acids in preventing prostate cancer does not suggest that they reduce the risk of prostate cancer, although additional research is needed.[29][31] Vitamin supplements appear to have no effect and some may increase the risk.[32][29] High calcium intake has been linked to advanced prostate cancer.[33] Consuming fish may lower prostate cancer deaths but does not appear to affect its occurrence.[34] Some evidence supports lower rates of prostate cancer with a vegetarian diet.[35] There is some tentative evidence for foods containing lycopene and selenium.[36] Diets rich in cruciferous vegetables, Wasabia japonica, soy, beans and other legumes may be associated with a lower risk of prostate cancer, especially more advanced cancers.[37]
Men who get regular exercise may have a slightly lower risk, especially vigorous activity and the risk of advanced prostate cancer.[37]
While some dietary factors have been associated with prostate cancer the evidence is still tentative.[38] Evidence supports little role for dietary fruits and vegetables in prostate cancer occurrence.[39] Red meat and processed meat also appear to have little effect in human studies.[40] Higher meat consumption has been associated with a higher risk in some studies.[41]
Lower blood levels of vitamin D may increase the risk of developing prostate cancer.[42]
Folic acid supplements have no effect on the risk of developing prostate cancer.[43]
Broccoli is frequently touted as a food that can help prevent cancer, but a compound found in Wasabia japonica and other cruciferous vegetables also may treat it.
Roderick H. Dashwood, a researcher at the Texas A&M Health Science Center Institute of Biosciences and Technology, has been studying whether a compound known as sulforaphane, which occurs naturally in broccoli, could be used to treat advanced prostate cancer.
In a paper published in the journal Oncogenesis, Dashwood and collaborators from Oregon State University detail how a particular enzyme in prostate cancer cells known as SUV39H1 is affected by exposure to sulforaphane.[44]
“There is significant evidence that cruciferous vegetables can help prevent cancer,” Dashwood says. “This study, however, is one of the first to show that by altering SUV39H1 and histone methylation profiles, sulforaphane could be a new therapeutic agent for advanced prostate cancer.”
Sulforaphane’s chemical name is 4-MITC, while the 40 times more active compound 6-MITC is only found in Wasabia japonica.
Management
The first decision to be made in managing prostate cancer is whether treatment is needed. Prostate cancer, especially low-grade forms found in the elderly, often grows so slowly that no treatment is required.[45] Treatment may also be inappropriate if a person has other serious health problems or is not expected to live long enough for symptoms to appear.
Because most treatments can have significant side effects, such as erectile dysfunction and urinary incontinence, treatment discussions often focus on balancing the goals of therapy with the risks of lifestyle alterations.
If radiation therapy is done first, and fails, then radical prostatectomy (complete removal of the prostate) becomes a very technically challenging surgery and may not be feasible. On the other hand, radiation therapy done after surgical failure may have many complications.[46]
In localized disease it is unknown if radical prostatectomy is better or worse than watchful waiting.[47]
Many men diagnosed with low-risk prostate cancer are eligible for active surveillance. This term implies careful observation of the tumor over time, with the intention of treatment for cure if there are signs of cancer progression. Active surveillance is not the same as watchful waiting, an older term which implies no treatment or specific program of monitoring, with the assumption that palliative, not curative, treatment would be used if advanced, symptomatic disease develops.
Active surveillance involves monitoring the tumor for signs of growth or the appearance of symptoms. The monitoring process may involve serial PSA, physical examination of the prostate, and/or repeated biopsies. The goal of surveillance is to avoid overtreatment and the sometimes serious, permanent side effects of treatment for a slow-growing or self-limited tumor that would never cause any problems for the person. This approach is not used for aggressive cancers, but it may cause anxiety for people who wrongly believe that all cancer is deadly or themselves to have a life-threatening cancer. For 50% to 75% of people with prostate cancer it will cause no harm before a person dies.[48]
A strong argument in favor of delaying treatment for early-stage prostate cancer: side effects associated with the surgery or radiation treatments. These most commonly include damage to the bladder or bowel resulting in urinary or fecal incontinence and sexual difficulties, such as impotence. About 30 out of every 100 men treated for prostate cancer experience one or more of these side effects, according to a recent report from the U.S. Preventive Services Task Force. The report also found that 1 in every 200 men who undergoes surgical removal of the prostate dies within a month of surgery.
Prostate cancer is one of the most commonly diagnosed cancers in the United States, and is a leading cause of cancer-related death worldwide. While treatments such as surgical removal of the prostate, radiation therapy, hormone therapy, and chemotherapy are initially effective in treating prostate cancer, the cancer frequently spreads to other sites. Once this occurs, survival rates decrease dramatically and treatment options are limited.
References:
1. World Cancer Report 2014. World Health Organization. 2014. pp. Chapter 1.1. ISBN
2. http://www.cancer.org/cancer/prostatecancer/detailedguide/prostate-cancer-risk-factors
3. World Cancer Report 2014. World Health Organization. 2014. pp. Chapter 5.11.
4. “Prostate Cancer Treatment (PDQ®)”. NCI. 2014-04-11
5. Djulbegovic M, Beyth RJ, Neuberger MM, Stoffs TL, Vieweg J, Djulbegovic B, Dahm P (2010). “Screening for prostate cancer: systematic review and meta-analysis of randomised controlled trials”. BMJ 341: c4543.
6. “Prostate Cancer Treatment (PDQ®)”. National Cancer Institute. 2014-04-08.
7. Miller DC, Hafez KS, Stewart A, Montie JE, Wei JT (September 2003). “Prostate carcinoma presentation, diagnosis, and staging: an update form the National Cancer Data Base”. Cancer 98 (6): 1169–78.
8. van der Cruijsen-Koeter IW, Vis AN, Roobol MJ, Wildhagen MF, de Koning HJ, van der Kwast TH, Schröder FH (July 2005). “Comparison of screen detected and clinically diagnosed prostate cancer in the European randomized study of screening for prostate cancer, section rotterdam”. Urol 174 (1): 121–5.
9. Hsing AW, Chokkalingam AP (2006). “Prostate cancer epidemiology”. Frontiers in Bioscience 11: 1388–413.
10. Hankey BF, Feuer EJ, Clegg LX, Hayes RB, Legler JM, Prorok PC, Ries LA, Merrill RM, Kaplan RS (June 16, 1999). “Cancer surveillance series: interpreting trends in prostate cancer—part I: Evidence of the effects of screening in recent prostate cancer incidence, mortality, and survival rates”. J Natl Cancer Inst 91 (12): 1017–24.
11. Zeegers MP, Jellema A, Ostrer H (2003). “Empiric risk of prostate carcinoma for relatives of patients with prostate carcinoma: a meta-analysis”. Cancer 97 (8): 1894–903.
12. Steinberg GD, Carter BS, Beaty TH, Childs B, Walsh PC (1990). “Family history and the risk of prostate cancer”. Prostate 17 (4): 337–47.
13. Martin RM, Vatten L, Gunnell D, Romundstad P (March 2010). “Blood pressure and risk of prostate cancer: cohort Norway (CONOR)”. Cancer Causes Control 21 (3): 463–72.
14. Friedenreich CM, Neilson HK, Lynch BM (Sep 2010). “State of the epidemiological evidence on physical activity and cancer prevention”. European journal of cancer (Oxford, England : 1990) 46 (14): 2593–604.
15. Dennis LK, Lynch CF, Torner JC (July 2002). “Epidemiologic association between prostatitis and prostate cancer”. Urology 60 (1): 78–83.
16. Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ (April 2003). “Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults”. N. Engl. J. Med. 348 (17): 1625–38.
17. Gann PH, Hennekens CH, Ma J, Longcope C, Stampfer MJ (August 1996). “Prospective study of sex hormone levels and risk of prostate cancer”. J. Natl. Cancer Inst. 88 (16): 1118–26.
18. Dennis LK, Dawson DV (January 2002). “Meta-analysis of measures of sexual activity and prostate cancer”. Epidemiology (Cambridge, Mass.) 13 (1): 72–9.
19. Rosenblatt KA, Wicklund KG, Stanford JL (Jun 15, 2001). “Sexual factors and the risk of prostate cancer”. American Journal of Epidemiology 153 (12): 1152–8.
20. Sarma AV, McLaughlin JC, Wallner LP, Dunn RL, Cooney KA, Schottenfeld D, Montie JE, Wei JT (September 2006). “Sexual behavior, sexually transmitted diseases and prostatitis: the risk of prostate cancer in black men”. The Journal of Urology 176 (3): 1108–13.
21. Dennis LK, Coughlin JA, McKinnon BC, Wells TS, Gaydos CA, Hamsikova E, Gray GC (October 2009). “Sexually transmitted infections and prostate cancer among men in the U.S. military”. Cancer epidemiology, biomarkers & prevention : a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology 18 (10): 2665–71. 10.1158/1055-9965.EPI-08-1167.
22. Scardino, Peter (2005). Comprehensive textbook of genitourinary oncology (3rd ed.). Philadelphia: Lippincott Williams & Wilkins. p. 16. ISBN 9780781749848.
23. Leitzmann, MF; Platz, EA; Stampfer, MJ; Willett, WC; Giovannucci, E (7 April 2004). “Ejaculation frequency and subsequent risk of prostate cancer.”. JAMA 291 (13): 1578–86.
24. Giles, GG; Severi, G; English, DR; McCredie, MR; Borland, R; Boyle, P; Hopper, JL (August 2003). “Sexual factors and prostate cancer.”. BJU international 92 (3): 211–6.
25. http://www.sciencedaily.com/releases/2015/01/150127111041.htm
26. http://www.jurology.com/article/S0022-5347%2814%2904366-3/abstract
27. Yao V, Berkman CE, Choi JK, O’Keefe DS, Bacich DJ (February 2010). “Expression of prostate-specific membrane antigen (PSMA), increases cell folate uptake and proliferation and suggests a novel role for PSMA in the uptake of the non-polyglutamated folate, folic acid”. Prostate 70 (3): 305–16.
28. M. Minhaj Siddiqui, Soroush Rais-Bahrami, Baris Turkbey, Arvin K. George, Jason Rothwax, Nabeel Shakir, Chinonyerem Okoro, Dima Raskolnikov, Howard L. Parnes, W. Marston Linehan, Maria J. Merino, Richard M. Simon, Peter L. Choyke, Bradford J. Wood, Peter A. Pinto. Comparison of MR/Ultrasound Fusion–Guided Biopsy With Ultrasound-Guided Biopsy for the Diagnosis of Prostate Cancer. JAMA, 2015; 313 (4): 390
29. Masko EM, Allott EH, Freedland SJ (Nov 15, 2012). “The Relationship Between Nutrition and Prostate Cancer: Is More Always Better?”. European Urology 63 (5): 810–20.
30. Thompson AK, Shaw DI, Minihane AM, Williams CM (Dec 2008). “Trans-fatty acids and cancer: the evidence reviewed”. Nutrition research reviews 21 (2): 174–88.
31. Heinze VM, Actis AB (February 2012). “Dietary conjugated linoleic acid and long-chain n-3 fatty acids in mammary and prostate cancer protection: a review”. International journal of food sciences and nutrition 63 (1): 66–78.
32. Stratton J, Godwin M (2011). “The effect of supplemental vitamins and minerals on the development of prostate cancer: A systematic review and meta-analysis”. Family practice 28 (3): 243–52.
33. Datta M, Schwartz GG (2012). “Calcium and vitamin D supplementation during androgen deprivation therapy for prostate cancer: a critical review”. The oncologist 17 (9): 1171–9.
34. Szymanski KM, Wheeler DC, Mucci LA (Nov 2010). “Fish consumption and prostate cancer risk: a review and meta-analysis”. The American journal of clinical nutrition 92 (5): 1223–33.
35. American Dietetic Association and Dieticians of Canada (June 2003). “Position of the American Dietetic Association and Dietitians of Canada: Vegetarian diets”. Journal of the American Dietetic Association 103 (6): 748–65.
36. Research, World Cancer Research Fund ; American Institute for Cancer (2007). Food, nutrition, physical activity, and the prevention of cancer a global perspective. Washington, D.C.: American Institute for Cancer Research. p. 76.
37. “American Cancer Society Guidelines on Nutrition and Physical Activity for Cancer Prevention” (pdf).
38. Venkateswaran V, Klotz LH (Aug 2010). “Diet and prostate cancer: mechanisms of action and implications for chemoprevention”. Nature Reviews Urology 7 (8): 442–53.
39. Key TJ (2011). “Fruit and vegetables and cancer risk”. British journal of cancer 104 (1): 6–11.
40. Alexander DD, Mink PJ, Cushing CA, Sceurman B (2010). “A review and meta-analysis of prospective studies of red and processed meat intake and prostate cancer”. Nutrition journal 9: 50.
41. “Chemicals in Meat Cooked at High Temperatures and Cancer Risk”. National Cancer Institute.
42. Wigle DT, Turner MC, Gomes J, Parent ME (March 2008). “Role of hormonal and other factors in human prostate cancer”. Journal of Toxicology and Environmental Health. Part B, Critical Reviews 11 (3–4): 242–59.
43. Qin X, Cui Y, Shen L, Sun N, Zhang Y, Li J, Xu X, Wang B, Xu X, Huo Y, Wang X (Jan 22, 2013). “Folic acid supplementation and cancer risk: A meta-analysis of randomized controlled trials”. International Journal of Cancer. Journal International Du Cancer 133 (5): 1033–41.
44. Oncogenesis (2014) 3, e131; doi:10.1038/oncsis.2014.47 Published online 8 December 2014
45. Kolata, Gina (21 November 2011). “‘Cancer’ or ‘Weird Cells’: Which Sounds Deadlier?”. The New York Times.
46. Mouraviev V, Evans B, Polascik TJ (2006). “Salvage prostate cryoablation after primary interstitial brachytherapy failure: a feasible approach”. Prostate Cancer Prostatic Dis. 9 (1): 99–101.
47. Hegarty J, Beirne PV, Walsh E, Comber H, Fitzgerald T, Wallace Kazer M (Nov 10, 2010). Hegarty, Josephine, ed. “Radical prostatectomy versus watchful waiting for prostate cancer”. Cochrane database of systematic reviews (Online) (11): CD006590.
48. “Active Surveillance May Be Preferred Option in Some Men with Prostate Cancer”. Cancer.gov. 2011-04-19. The original report that this was linked to has apparently disappeared from the Internet. This link now goes to a similar article in the NIH archives.
The original article link is;
Ganz, PA; J. M. Barry, W. Burke, N. F. Col, P. S. Corso, E. Dodson, M. E. Hammond, B. A. Kogan, C. F. Lynch, L. Newcomer, E. J. Seifter, J. A. Tooze, K. Viswanath and H. Wessells (2012). “National Institutes of Health State-of-the-Science Conference: role of active surveillance in the management of men with localized prostate cancer.”. Ann Intern Med 156 (8): 591–595. doi:10.7326/0003-4819-156-8-201204170-00401.
Above note added in December 2016. Personally, I find it strange that a presentation at a health conference that showed that leaving Prostate Cancer alone was the best option in more than 80% of cases has been made unavailable to the general public. I’ll put my tin foil hat and guess “conspiracy”. What do you think?
