
Ovarian Cancer is 5th most common cancer for women.
This is a cancer that is purely limited to females, our wives, mothers, sisters and other female relatives, lovers, colleagues and acquaintances.
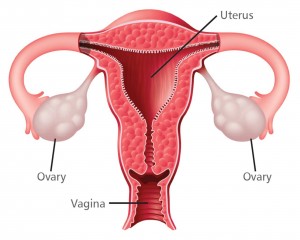
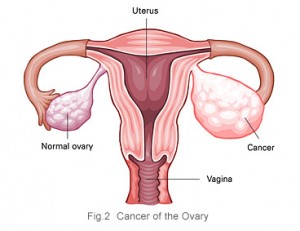
Ovarian cancer begins in an ovary and can spread to other parts of the body. The ovaries are part of the female reproductive system. They produce a woman’s eggs and female hormones. Each ovary is about the size and shape of an almond.
It’s the fifth most common cancer among women after lung cancer, breast cancer, bowel / colon cancer, and cancer of the uterus (womb).
Ovarian cancer is most common in women who have been through the menopause (usually over the age of 50), although it can affect women of any age. The cause is unknown.
Signs and symptoms of ovarian cancer are frequently absent in early stages and when they exist, they may be subtle. In most cases, the symptoms persist for several months before being recognized and diagnosed, or they may be misdiagnosed as a condition such as irritable bowel syndrome.[1] It is for this reason that ovarian cancer is rarely diagnosed until it has grown to a life threatening stage.
As the symptoms of ovarian cancer can be similar to those of other conditions, it can be difficult to recognise. However, there are early symptoms to look out for, such as persistent bloating, pain in the pelvis and lower stomach, and difficulty eating.
Women with ovarian cancer may have no symptoms or just mild symptoms until the disease is in an advanced stage. Then it is hard to treat. Symptoms may include
- A heavy feeling in the pelvis
- Pain in the lower abdomen
- Bleeding from the vagina
- Weight gain or loss
- Abnormal periods
- Unexplained back pain that gets worse
- Gas, nausea, vomiting, or loss of appetite
To diagnose ovarian cancer, doctors do one or more tests. They include a physical exam, a pelvic exam, lab tests, ultrasound, or a biopsy. Treatment is usually surgery followed by chemotherapy.
See your doctor if you have the following symptoms on a daily basis for more than a few weeks:
- Bloating or swollen belly area
- Difficulty eating or feeling full quickly (early satiety)
- Pelvic or lower abdominal pain; the area may feel “heavy” (pelvic heaviness)
When diagnosed, the preferred method of dealing with it is to cut it out. This normally involves removing the ovary or ovaries, and can include a complete hysterectomy – a total removal of all female reproductive organs.
Long periods of continuous ovulation are thought to be the main non-genetic cause of ovarian cancer. This is because the cells are constantly stimulated to divide while egg production cycles continue. Therefore, people who have not borne children are at twice the risk of ovarian cancer than people who have had children.
The suppression of ovulation through the use of birth control pills appears to be useful in reducing the risk of ovarian cancer. There are the long term effects of taking these drugs to be considered, such as increasing the risk of breast and cervical cancer.[4]
If caught and treated in an early stage, ovarian cancer may (my emphasis) be curable. Treatments usually include some combination of surgery, radiation therapy, or chemotherapy.[2] Outcomes depend on the extent of the disease and the subtype of cancer present.[3] The overall five-year survival rate in the United States is 45%.[5] Outcomes are worse in the developing world.[3]
On a worldwide basis it is the seventh-most common cancer and the fifth-most common cause of death from cancer in women. It is more common in North America and Europe than Africa and Asia.[3]
Risk factors
Most of the risk factors for ovarian cancer are hormonal in nature. Not having children is a risk factor for ovarian cancer, likely because ovulation is not suppressed due to pregnancy. Both obesity and hormone replacement therapy raise the risk for ovarian cancer.[6]
Postmenopausal hormone replacement therapy (HRT) with estrogen likely increases the risk of ovarian cancer, but the association has not been confirmed in a large-scale study.[7][8] However, notable studies including the Million Women Study have supported this link. Postmenopausal HRT with combined estrogen and progesterone may increase risk if used for over 5 years, but this risk returns to normal after cessation of therapy.[9]
In the United States, five of 100 women with a first-degree relative with ovarian cancer will eventually get ovarian cancer themselves, triple the risk of women with unaffected family members. Seven of 100 women with two or more relatives with ovarian cancer will eventually get ovarian cancer.[7][10] In general, 5-10% of ovarian cancer cases have a genetic cause.[7]
Young girls and adolescents with suspected ovarian tumors need to be diagnosed as early as possible, because the younger the patient, the greater the likelihood of a malignant tumor.
Environmental factors
Industrialized nations, with the exception of Japan, have high rates of ovarian cancer, which may be due to diet in those countries. White people are at a 30-40% higher risk for ovarian cancer when compared to Black and Hispanic people, likely due to socioeconomic factors: White women have fewer children and different rates of gynecologic surgeries that affect risk for ovarian cancer.[7]
Smoking tobacco is associated with a higher risk of mucinous ovarian cancer; after smoking stops, the risk eventually returns to normal.[9]
Protective factors
Stopping the release of an egg from the ovary, which damages the outer layer of the ovary, and its associated inflammation, is generally protective. This effect can be achieved by having children, taking combined oral contraceptives, and breast feeding, all of which are protective factors.[6] A longer period of breast feeding decreases the risk of ovarian cancer more.[9] Each birth decreases risk of ovarian cancer more, and this effect is seen with up to five births. Combined oral contraceptives reduce the risk of ovarian cancer by up to 50%, and the protective effect of combined oral contraceptives can last 25-30 years after they are discontinued.[7][9]
A diet that includes large amounts of carotene, fibre, and vitamins with low amounts of fat may be protective.[7] Specifically, a diet with non-starchy vegetables (e.g. wasabi, cabbage family and onions) may help to reduce risk of ovarian cancer, but research is still ongoing in this area.[9]
To definitively diagnose ovarian cancer, a surgical procedure to inspect the abdomen is required. This can be an open procedure (laparotomy, incision through the abdominal wall) or keyhole surgery (laparoscopy). During this procedure, suspicious areas are removed and sent for microscopic analysis.
Screening
The only screening recommended for all women is an annual pelvic examination. This is not very effective in detecting early ovarian cancer because it is usually only able to be touched or felt in advanced stages.[7] Ovarian cancer screening is of high clinical interest because the disease is not typically detectable at its early stages, when it is the most curable.
Ovarian cancer is not very common, even in the high-risk group of women from the ages of 50 to 60 (about one in 2000), and screening of women with average risk is more likely to give ambiguous results than detect a problem which requires treatment. Because ambiguous results are more likely than detection of a treatable problem, and because the usual response to ambiguous results is invasive surgeries, in women of average risk, the potential harms of having screening without an indication outweigh the potential benefits.
Prevention
Since no one knows what causes ovarian cancer, prevention tends to be hit and miss. Apart from having children and taking oral contraceptives, most prevention methods are just guesswork.
People with strong genetic risk for ovarian cancer may consider the surgical removal of their ovaries as a preventative measure. This is often done after completion of childbearing years. This reduces the chances of developing both breast cancer (by around 50%) and ovarian cancer (by about 96%) in people at high risk.
Treatment usually involves chemotherapy and surgery, and sometimes radiotherapy. Surgical treatment may be sufficient for well-differentiated malignant tumours and confined to the ovary. Addition of chemotherapy may be required for more aggressive tumours confined to the ovary. For patients with advanced disease, a combination of surgical reduction with a combination chemotherapy regimen is standard. Borderline tumours, even following spread outside of the ovary, are managed well with surgery, and chemotherapy is not seen as useful.
Ovarian cancer usually has a relatively poor survival rate. It is disproportionately deadly because it lacks any clear early detection or screening test, meaning most cases are not diagnosed until they have reached advanced stages.[11] However, in some cases, ovarian cancer recurrences can be treated successfully.[1]
More than 60% of women presenting with ovarian cancer have stage-III or stage-IV cancer, when it has already spread beyond the ovaries.
Ovarian cancer frequently recurs after treatment. If a recurrence occurs in advanced disease, it typically occurs within 18 months of initial treatment (18 months progression-free survival). Recurrences can be treated, but the disease-free interval tends to shorten and chemo-resistance increases with each recurrence.[1] Low malignant potential tumours rarely relapse, even when fertility-sparing surgery is the treatment of choice.
New development
In addition to Wasabia japonica being able to kill most cancer cells, another natural product has been found that actively attacks later stage ovarian cancer cells. More information can be found here.
References
1. Jayson GC, Kohn EC, Kitchener HC, Ledermann JA (October 2014). “Ovarian cancer”. Lancet 384 (9951): 1376–88.
2. “Ovarian Epithelial Cancer Treatment (PDQ®)”. NCI. 2014-05-12.
3. World Cancer Report 2014. World Health Organization. 2014. pp. Chapter 5.12.
4. http://www.cancer.gov/cancertopics/factsheet/Risk/oral-contraceptives
5. “SEER Stat Fact Sheets: Ovary Cancer”. NCI.
6. Seiden, Michael V. (2012). “Gynecologic Malignancies”. In Longo DL, Kasper DL, Jameson JL, Fauci AS, Hauser SL, Loscalzo J. Harrison’s Principles of Internal Medicine (18th ed.). McGraw-Hill.
7. Hoffman, Barbara L.; Schorge, John O.; Schaffer, Joseph I.; Halvorson, Lisa M.; Bradshaw, Karen D.; Cunningham, F. Gary (2012). “Epithelial Ovarian Cancer”. Williams Gynecology (2nd ed.). McGraw Hill Medical. pp. 853–878.
8. Manson, JoAnn E.; Bassuk, Shari S. (2012). “The Menopause Transition and Postmenopausal Hormone Therapy”. In Longo DL, Kasper DL, Jameson JL, Fauci AS, Hauser SL, Loscalzo J. Harrison’s Principles of Internal Medicine (18th ed.). McGraw-Hill.
9. “Ovarian cancer risks and causes”. Cancer Research UK. 15 January 2014.
10. “Ovarian Cancer Prevention (PDQ®)”. National Cancer Institute. 2013
11. Society of Gynecologic Oncology (February 2014), “Five Things Physicians and Patients Should Question”, Choosing Wisely: an initiative of the ABIM Foundation (Society of Gynecologic Oncology)
Here is another interesting take (with pictures) on this very subject.

Update for my wife Sylvia who has Stage IV Ovarian Cancer (Diagnosed Jan. 2013).
Almost two months ago, she started taking 2 drops of Frankensence Oil from Africa in 8 oz of water, along with 3 capsuls of your Wasabi Root Powder.
First 3 weeks: CA 125 dropped from 143 – 118
2nd 3 weeks: CA 125 dropped from 118 – 84 (last MOnday.
Good results here. Keep up the good work!
David
[Editor: Blood test, which can detect a protein (CA 125) found on the surface of ovarian cancer cells.]